Hyperplastic polyps are usually small, located in the end-portion of the colon (the rectum and sigmoid colon), have no potential to become malignant, and are not worrisome. It is not always possible to distinguish a hyperplastic polyp from an adenomatous polyp based upon appearance during colonoscopy, which means that hyperplastic polyps are often removed or biopsied to allow microscopic examination.
Two-thirds of colon polyps are adenomas. Most of these polyps do not develop into cancer, although they have the potential to become cancerous. Adenomas are classified by their size, general appearance, and specific features as seen under the microscope.
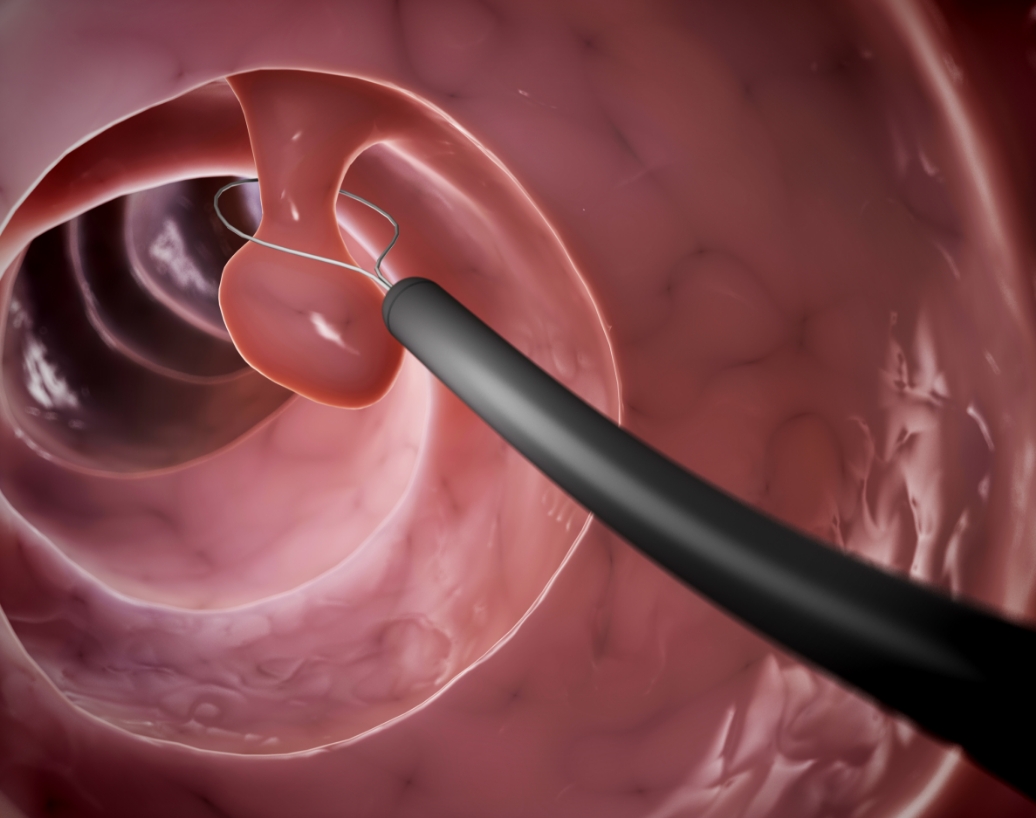
As a general rule, the larger the adenoma, the more likely it is to eventually become a cancer. As a result, large polyps (larger than 5 millimeters) are usually removed completely to prevent cancer and for microscopic examination to guide follow-up testing.
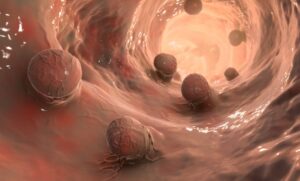
Polyps that contain cancerous cells are known as malignant polyps. The optimal treatment for malignant polyps depends upon the extent of the cancer (when examined with a microscope) and other individual factors.